What Causes BPPV? Why Did I Get Vertigo Out of Nowhere?
One of the most common questions I hear at Prime ENT Center is: “Dr. Porwal, WHY did this happen to me? I was fine yesterday and today I can’t even get out of bed without the room spinning!”
It’s frustrating, I know. BPPV (Benign Paroxysmal Positional Vertigo) often strikes out of the blue, and understanding what caused it can help you make sense of what you’re going through—and maybe even prevent it from happening again.
So let’s talk about what actually causes those tiny calcium crystals in your inner ear to break loose and wreak havoc on your balance system.
📞 Experiencing Sudden Vertigo?
Dr. Prateek Porwal can diagnose and treat BPPV same-day at Prime ENT Center, Hardoi
Call: 7393062200
📍 Serving Hardoi, Lucknow, Kanpur, Unnao, Sitapur
The Root Cause: Loose Otoconia Crystals
Before we talk about WHY the crystals break loose, let’s quickly review WHAT’S happening in your inner ear.
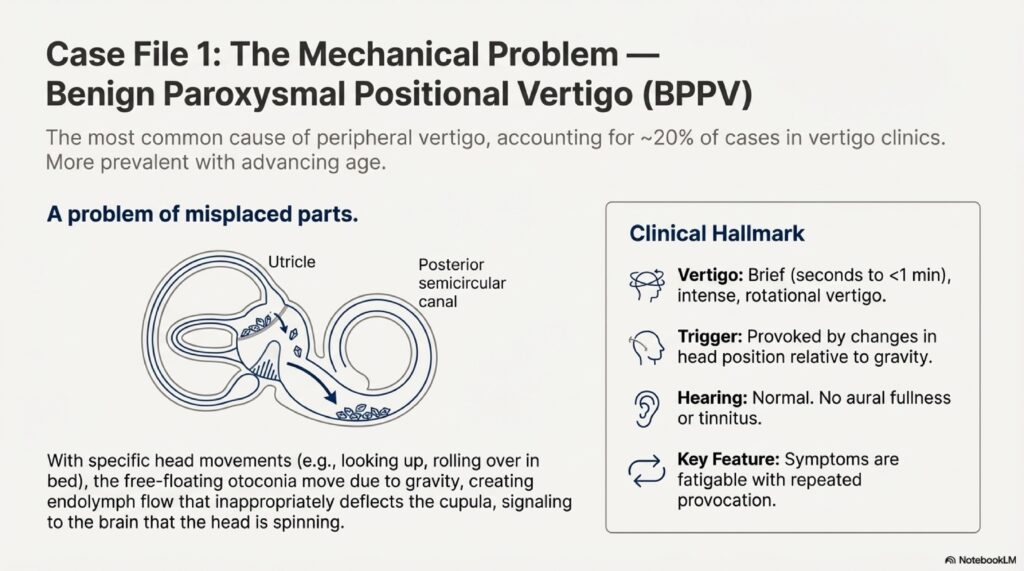
Your inner ear contains tiny calcium carbonate crystals called otoconia (or otoliths). Normally, these crystals live in a structure called the utricle, stuck to a gel-like membrane. They help you sense gravity and linear acceleration—like when you’re in an elevator or a car that’s speeding up.
In BPPV, some of these crystals break free from the utricle and migrate into one of your semicircular canals (usually the posterior canal). These canals are designed to sense rotational movement, NOT the presence of heavy calcium crystals floating around. When you move your head, the crystals tumble through the canal, creating abnormal fluid motion that your brain misinterprets as intense spinning.
So the real question is: Why do the otoconia crystals break loose in the first place?
Known Causes of BPPV
1. Head Trauma (Even Minor)
About 7-17% of BPPV cases follow some kind of head injury. And we’re not just talking about major trauma—even relatively minor bumps can dislodge otoconia.
Examples I’ve seen:
- Car accidents (even minor fender-benders where you didn’t hit your head hard)
- Falls where you bumped your head
- Sports injuries (getting hit in the head with a ball, collision with another player)
- Dental work that involved prolonged head-back positioning
- Whiplash injuries
The mechanism makes sense—a sudden jolt can literally shake the crystals loose from their gel membrane, like shaking snow off a tree branch.
Post-traumatic BPPV tends to affect younger people (who are more active and prone to head injuries) and is more likely to involve multiple canals or both ears.
2. Viral Inner Ear Infections
Vestibular neuritis or labyrinthitis (viral infections of the inner ear) can damage the utricle’s structure, making it easier for crystals to break free later. I’d say about 15% of BPPV cases I see follow an episode of acute vertigo from vestibular neuritis.
What happens is the virus causes inflammation that damages the otolithic membrane. Even after the infection resolves, the weakened membrane can’t hold onto the crystals as well, and weeks or months later—boom, BPPV develops.
3. Meniere’s Disease
About 30% of people with Meniere’s disease eventually develop BPPV. The endolymphatic hydrops (fluid buildup) in Meniere’s can damage the utricle and cause crystal degeneration.
If you have both Meniere’s AND BPPV, it can be particularly confusing because you’re dealing with two different types of vertigo with different triggers and treatments.
4. Migraine
There’s an interesting connection between vestibular migraine and BPPV. People with migraines seem to have higher rates of BPPV, possibly because migraines cause changes in inner ear blood flow or chemistry that weaken the otolithic membrane.
I often see patients who have both vestibular migraine AND BPPV, which can be diagnostically challenging.
5. Prolonged Bed Rest or Immobilization
This is fascinating—people who’ve been bedridden for extended periods (after surgery, during illness, etc.) have higher rates of BPPV when they finally get up and move around.
The theory is that:
- Lack of head movement allows crystals to settle and potentially detach
- Reduced blood flow to the inner ear during prolonged immobility
- Possible demineralization of the otolithic membrane
I saw this a lot during COVID when people were laid up in hospital beds for weeks. Once they recovered and started moving around—BPPV.
6. Ear Surgery or Procedures
Any surgery or procedure involving the ear can potentially trigger BPPV:
- Stapedectomy (for otosclerosis)
- Cochlear implantation
- Mastoidectomy
- Even ear canal irrigation or wax removal (rare, but I’ve seen it)
The mechanical disruption during surgery can shake crystals loose.
7. Osteoporosis and Vitamin D Deficiency
Here’s where it gets interesting. Recent research shows that people with osteoporosis and vitamin D deficiency have significantly higher rates of BPPV.
The otoconia are made of calcium carbonate, and their structure depends on normal calcium metabolism. When you have osteoporosis or low vitamin D:
- The crystals may become more fragile and break apart more easily
- The otolithic membrane may weaken
- New crystal formation after degeneration may be impaired
I now routinely check vitamin D levels in my recurrent BPPV patients, and I’d say about 60-70% of them are deficient. Supplementation doesn’t cure BPPV, but it might reduce recurrence.
8. Age-Related Degeneration
Let’s be honest—a lot of BPPV is just age-related wear and tear. The otolithic membrane degenerates naturally as we get older, making crystal detachment more likely.
BPPV is rare in children and young adults (unless there’s trauma), becomes more common after age 50, and peaks in the 60-80 age range. It’s one of those annoying things that happens as we age, like presbyopia or gray hair.
Idiopathic BPPV: When There’s No Clear Cause
Here’s the frustrating part: about 50-70% of BPPV cases are “idiopathic,” which is medical speak for “we have no idea why it happened.”
You didn’t hit your head. You haven’t been sick. You’re not on bed rest. You just woke up one morning and couldn’t move without spinning. Why?
Honestly, we don’t always know. It could be:
- Spontaneous degeneration of the otolithic membrane (age-related)
- Subclinical vitamin D deficiency
- Very minor head movements you don’t even remember
- Natural crystal turnover and replacement process gone wrong
- Genetic factors (BPPV does seem to run in families)
The good news? Idiopathic BPPV responds just as well to treatment as BPPV with a known cause. The Epley or BBQ Roll maneuver works regardless of why the crystals broke loose.
Risk Factors for Developing BPPV
While we can’t always pinpoint the exact cause, certain factors increase your risk:
Age Over 50
The older you are, the higher your risk. BPPV affects about 2-3% of the general population, but that jumps to 10% in people over 65 and nearly 50% by age 80. Aging is the single biggest risk factor.
Female Gender
Women are about 2-3 times more likely to develop BPPV than men. This might be related to:
- Hormonal factors (estrogen affects calcium metabolism)
- Higher rates of osteoporosis in women
- Possibly higher rates of migraine in women
I definitely see more women than men with BPPV in my clinic—probably 70-75% of my BPPV patients are female.
Osteoporosis
People with osteoporosis have about 1.5-2x higher risk of BPPV. The same process that weakens your bones may also affect the calcium carbonate crystals in your inner ear.
Vitamin D Deficiency
Low vitamin D levels are strongly associated with BPPV, especially recurrent BPPV. Some studies show that vitamin D supplementation reduces recurrence rates, though the evidence is still being debated.
History of Head Trauma
Even old head injuries increase your risk. I’ve had patients develop BPPV years after a concussion or car accident.
Migraine
Migraineurs have about 3-4x higher risk of BPPV compared to people without migraines.
Inner Ear Disorders
Having Meniere’s disease, vestibular neuritis, or labyrinthitis increases BPPV risk substantially.
🏥 Concerned About Your BPPV Risk?
Get comprehensive evaluation and treatment at Prime ENT Center
📞 Call 7393062200
Dr. Porwal can assess your risk factors and discuss prevention strategies
Can You Prevent BPPV?
This is the million-dollar question. Honestly, there’s no guaranteed way to prevent BPPV, especially the idiopathic type. But there are some things that might help:
Vitamin D Supplementation
If you’re deficient (which many people are), taking vitamin D supplements might reduce your risk of recurrence. I usually recommend 1000-as prescribed by your doctor, but check with your doctor and get your levels tested first.
Calcium and Bone Health
Maintaining good bone health with adequate calcium intake, weight-bearing exercise, and osteoporosis treatment (if needed) might help. Though the evidence here is less strong than for vitamin D.
Avoiding Prolonged Immobilization
If you’re recovering from surgery or illness and need bed rest, try to move your head around periodically (if medically safe). Don’t stay in one position for hours on end.
Treating Underlying Conditions
If you have Meniere’s disease, vestibular migraine, or other inner ear disorders, getting these well-controlled might reduce BPPV risk.
Head Protection
Wear helmets when biking, skiing, or doing other activities with head injury risk. Protect your head from falls, especially if you’re elderly.
Reality check: Even with all these precautions, you might still develop BPPV. It’s often just bad luck. The good news is it’s highly treatable.
Why Does BPPV Keep Coming Back?
About 15% of people who have BPPV will have a recurrence within one year. By 5 years, nearly 50% will have had at least one recurrence. This is incredibly frustrating for patients.
Why recurrence is common:
- The underlying problem (otolithic membrane degeneration) wasn’t fixed, just the symptoms
- New crystals can break loose at any time
- Risk factors (age, vitamin D deficiency, etc.) persist
- The treatment (Epley maneuver) repositions crystals but doesn’t prevent new ones from forming
Reducing recurrence risk:
- Vitamin D supplementation if deficient
- Calcium supplementation (though evidence is mixed)
- Vestibular rehabilitation exercises (might help retrain balance system)
- Treating underlying conditions
If you have very frequent recurrences (monthly or more), we might need to investigate for underlying causes like Meniere’s disease or consider other treatment options like canal plugging surgery (though this is very rare).
Common Myths About BPPV Causes
Myth: BPPV is caused by stress
Reality: Stress doesn’t directly cause BPPV. However, stress can trigger vestibular migraine, which might be confused with BPPV. Also, stress might make you more aware of mild BPPV symptoms you’d otherwise ignore.
Myth: Sleeping on one side causes BPPV
Reality: Your sleeping position doesn’t cause BPPV. However, you might NOTICE symptoms more when rolling in bed, which is when positional vertigo is triggered.
Myth: Ear wax causes BPPV
Reality: Ear wax is in your ear canal; BPPV crystals are deep in your inner ear. They’re completely unrelated. (Though ear irrigation to remove wax CAN rarely trigger BPPV due to the pressure changes.)
Myth: High blood pressure causes BPPV
Reality: There’s no direct connection. High blood pressure can cause dizziness through other mechanisms, but not BPPV specifically.
Myth: You can “catch” BPPV from someone
Reality: BPPV is not contagious! It’s a mechanical problem with your own inner ear crystals.
When to Worry: Red Flags
Most BPPV is benign (that’s literally in the name!). But occasionally, what seems like BPPV is actually something more serious. See a doctor urgently if you have:
- Constant vertigo (not positional—it doesn’t matter how you move your head)
- Hearing loss in one or both ears
- Neurological symptoms: double vision, slurred speech, weakness, numbness
- Severe headache with vertigo
- Inability to walk due to imbalance
- Vertigo lasting hours without stopping
- First episode after age 60 (could be stroke mimicking BPPV)
These symptoms suggest central causes (stroke, MS, tumor) rather than BPPV, and you need imaging (MRI) and neurological evaluation.
FAQs About BPPV Causes
Q: Can sleeping wrong cause BPPV?
A: No, sleeping position doesn’t cause BPPV. You might notice symptoms when you roll over in bed, but that’s triggering existing BPPV, not causing it.
Q: Can flying cause BPPV?
A: Pressure changes during flying don’t typically cause BPPV. However, you might notice BPPV symptoms during a flight because of head movements while navigating the plane or turbulence.
Q: Is BPPV hereditary?
A: There seems to be a familial component—BPPV runs in families more than would be expected by chance. But it’s not a simple genetic condition. Family history increases your risk but doesn’t guarantee you’ll get it.
Q: Can dental work cause BPPV?
A: Yes, actually! Prolonged head-back positioning in the dentist’s chair can trigger BPPV, especially if you already have loose crystals that haven’t caused symptoms yet. I’ve had several patients develop BPPV right after dental procedures.
Q: Does caffeine cause BPPV?
A: No, caffeine doesn’t cause BPPV. However, if you have vestibular migraine along with BPPV, caffeine might trigger the migraine component.
Q: Can allergies cause BPPV?
A: Allergies don’t directly cause BPPV. But severe allergies can cause Eustachian tube dysfunction and middle ear fluid, which might make you feel dizzy for different reasons.
🎯 Get Expert BPPV Diagnosis & Treatment
Understanding the cause helps, but treating the symptoms is what matters
📞 Call 7393062200 for same-day appointment
🌐 Book Online: drprateekporwal.com
📍 Prime ENT Center, Hardoi, UP
Dr. Prateek Porwal | Fellowship-Trained Vestibular Specialist
Related Articles
- BPPV Symptoms: How to Know If You Have It
- Epley Maneuver: Treatment That Actually Works
- Can You Prevent BPPV From Coming Back?
- Vitamin D and BPPV: What’s the Connection?
Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice, diagnosis or prescribing guidance. Consult Dr. Prateek Porwal at Prime ENT Center, Hardoi for personalised treatment.