You wake up dizzy. The room is spinning, you can’t stand straight, and you’re genuinely scared. Is this just vertigo, or is it something dangerous like a stroke? This is exactly the kind of patient I see regularly in my clinic, and the HINTS exam is one of my most important tools for answering this question quickly.
📋 Table of Contents
- What Is the HINTS Exam?
- The Three Parts of HINTS
- H = Head Impulse Test
- I = Nystagmus Direction
- T = Test of Skew
- The INFARCT Rule
- Who Actually Needs the HINTS Exam?
- What About MRI? Doesn’t That Rule Out Stroke?
- What About Other Causes? What If HINTS Is Normal But I’m Still Worried?
- My Clinical Experience
- The Bottom Line
- Need a Vertigo Evaluation?
- FAQ Schema
- What does HINTS stand for?
- Is HINTS exam more accurate than MRI for acute vertigo?
- What does a positive head impulse test mean?
- When should I get HINTS exam done?
- Can vertical nystagmus indicate a stroke?
- What is skew deviation in the Test of Skew?
- About Dr. Prateek Porwal
- References
The HINTS exam can be done in under a minute at the bedside, no machines, no waiting. It’s literally saved me from missing serious cases and, equally important, from ordering unnecessary MRIs when a patient just has benign vertigo.
What Is the HINTS Exam?
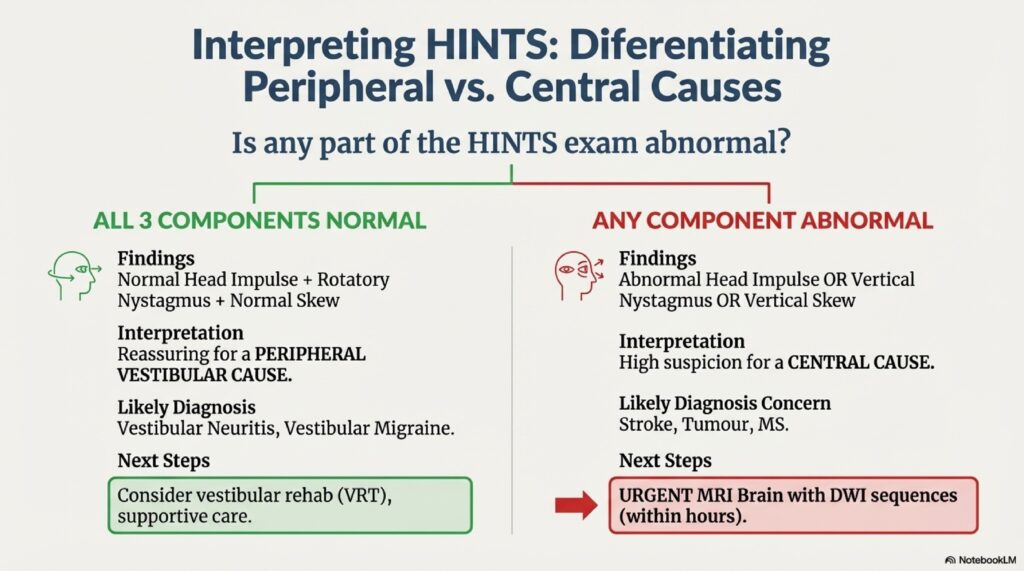
HINTS stands for Head Impulse, Nystagmus, Test of Skew. It’s a three-part bedside examination designed to tell the difference between a dangerous central cause of vertigo (like a brainstem stroke) and a harmless peripheral cause (like vestibular neuritis or BPPV).
The beauty of this test is that it’s actually more accurate than an immediate MRI in the first 48 hours of symptoms. I know that sounds counterintuitive, but it’s true. A normal MRI doesn’t rule out stroke in the first 24 hours, the stroke might be too small to see yet. But an abnormal HINTS exam tells me right now that something central is happening.
The Three Parts of HINTS
H = Head Impulse Test
This is the simplest part. I sit the patient in front of me and ask them to look at my nose. Then I move their head side to side, about 15-20 degrees, very quickly. The patient’s eyes should stay locked on my nose.
In a patient with peripheral vestibular loss (like vestibular neuritis or BPPV), the eyes will slip backward because the vestibulo-ocular reflex is weak. This is called a “positive head impulse”, and actually, in peripheral vertigo, this is normal and expected.
👉 Also read: Vertigo Specialist for Kolkata Patients — Dr. Prateek Porwal
But if the head impulse is normal, meaning the eyes stay locked on my nose, and the patient still has severe vertigo? That’s worrisome. It suggests a central cause, not a peripheral one.
I = Nystagmus Direction
Nystagmus is the involuntary eye movement patients get during vertigo. I’m looking for specific patterns. In peripheral vertigo, the nystagmus follows certain rules, it’s usually rotatory or horizontal, and it beats away from the affected side.
But in a central cause like brainstem stroke, the nystagmus can be vertical, purely vertical, or it changes direction depending on which way the patient looks (gaze-evoked). These are the kinds of nystagmus patterns that make me immediately think “this patient needs imaging and possibly admission.”
T = Test of Skew
This is where I check for a vertical misalignment of the eyes, a “skew deviation.” I cover one of the patient’s eyes for a few seconds, then uncover it and watch if that eye has to jump up or down to re-fixate.
If I see skew deviation, it suggests a midbrain or medullary problem. It’s not always present in strokes, but when it is, it’s a red flag.
👉 Also read: Vertigo Doctor Near Bareilly — Online &
The INFARCT Rule
Someone came up with the mnemonic INFARCT to help remember when a HINTS exam suggests central pathology:
- Impaired head impulse (normal reflexes in central disease)
- Nystagmus that’s vertical or gaze-evoked
- Fixation instability
- Abnormal vertical saccades
- Reflex skew deviation
- Cranial nerve findings
- Trigger of central symptoms
If any of these are present, the patient likely needs imaging and hospital admission. If none are present, and the head impulse is positive? The patient probably has peripheral vertigo.
Who Actually Needs the HINTS Exam?
I use HINTS for patients with acute vestibular syndrome, sudden onset of vertigo with imbalance and nystagmus. This usually means:
- Less than 7 days of symptoms
- Severe symptoms (can’t stand or walk without help)
- Spontaneous nystagmus present
- Imbalance on the head thrust test
I don’t need HINTS for BPPV because the clinical presentation is so distinctive (brief spinning attacks, head-dependent symptoms). And for mild peripheral vertigo with obvious causes, HINTS might be overkill.
But for any 60-year-old with sudden onset dizziness? I’m doing HINTS immediately. The risk of missing a stroke is just too high.
👉 Also read: Vertigo Specialist Near Lucknow, Dr. Prateek Porwal,
What About MRI? Doesn’t That Rule Out Stroke?
Here’s the honest answer: not in the first 24 hours. Diffusion-weighted imaging (DWI) MRI is the gold standard for detecting acute stroke, but it can miss small brainstem strokes up to 30% of the time in the first 48 hours. The lesion is just too small.
So I explain to my patients: if your HINTS exam is abnormal, you need imaging and hospital admission now. Don’t wait for an MRI. If your HINTS exam is normal, an MRI is less urgent, and most likely won’t change management anyway.
This is actually how major hospitals use HINTS, it’s part of the acute stroke workup in emergency departments. The test is good enough to make immediate decisions.
What About Other Causes? What If HINTS Is Normal But I’m Still Worried?
Fair question. A normal HINTS exam is very reassuring for excluding acute central stroke, but it doesn’t rule out everything. Things like Wallenberg syndrome (lateral medullary stroke) might have subtle findings on HINTS. Some posterior circulation strokes can have minimal findings.
That’s why clinical judgment matters. If a patient has red flags like:
👉 Also read: Diagnosis of Vertigo
- Sudden onset with headache or neck pain
- History of stroke or atrial fibrillation
- Focal neurological signs (weakness, speech difficulty, facial drooping)
- Abnormal reflexes or cranial nerve findings
Then I’m getting an MRI regardless of HINTS results. The test is a tool, not a crystal ball.
My Clinical Experience
I’ve been using HINTS for years now, and it’s saved me more than once. I had a 58-year-old man come in with severe vertigo. His family was sure it was a stroke. His HINTS exam was completely normal, positive head impulse, horizontal nystagmus, no skew. I reassured him and his family that this looked like peripheral vertigo. We did labs, got an MRI the next day (which was normal), and diagnosed him with vestibular neuritis. He’s fine now.
Then there was the 65-year-old woman who came in looking like textbook BPPV with complaints of dizziness. But her HINTS exam was abnormal, vertical nystagmus, normal head impulse. MRI showed a small cerebellar stroke. She got admitted to the hospital, got appropriate treatment, and did well.
That’s why I never skip HINTS anymore.
The Bottom Line
The HINTS exam is a powerful tool that any doctor should know how to do. It’s faster, more sensitive, and more specific than early MRI for detecting central vertigo in the acute phase. It takes literally 60 seconds and requires nothing but your hands and eyes.
👉 Also read: Is Vertigo Curable Permanently? An ENT Doctor Answers Honestly
If you’re having sudden severe vertigo, ask your doctor if they’ve checked your HINTS. If they don’t know what that means, push for it or get to an emergency department where they do. Early identification of central causes changes everything.
Need a Vertigo Evaluation?
If you’re experiencing sudden dizziness or vertigo, I’d recommend a proper evaluation. Call me at 7393062200 or WhatsApp https://wa.me/917393062200 to book an appointment at Prime ENT Center in Hardoi.
FAQ Schema
What does HINTS stand for?
HINTS stands for Head Impulse, Nystagmus, Test of Skew, a three-part bedside exam that differentiates peripheral vertigo from central (stroke-related) vertigo.
Is HINTS exam more accurate than MRI for acute vertigo?
For detecting acute central vertigo in the first 48 hours, HINTS is actually more sensitive than MRI because MRI can miss small brainstem strokes that are too small to visualize initially.
What does a positive head impulse test mean?
A positive head impulse (eyes slip backward during rapid head movement) suggests peripheral vestibular loss and is reassuring for excluding central stroke in the context of other normal HINTS findings.
When should I get HINTS exam done?
Any patient with acute onset severe vertigo (less than 7 days) with spontaneous nystagmus and imbalance should have HINTS performed to rule out dangerous central causes.
Can vertical nystagmus indicate a stroke?
Yes, vertical nystagmus or gaze-evoked nystagmus on HINTS examination suggests central pathology like brainstem stroke and requires immediate MRI and hospital admission.
What is skew deviation in the Test of Skew?
Skew deviation is a vertical misalignment of the eyes that suggests midbrain or medullary pathology. It’s detected by the cover test, watching if one eye jumps vertically when uncovered.
About Dr. Prateek Porwal
Dr. Prateek Porwal is an ENT & Vertigo Specialist with over 13 years of experience, holding MBBS (GSVM Medical College), DNB ENT (Tata Main Hospital), and CAMVD (Yenepoya University). He is the originator of the Bangalore Maneuver for Anterior Canal BPPV and has published research in Frontiers in Neurology and IJOHNS. Serving at Prime ENT Center, Hardoi.
Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice, diagnosis or prescribing guidance. All medications must be taken under direct supervision of a qualified physician. Consult Dr. Prateek Porwal at Prime ENT Center, Hardoi for personalised treatment.
References
- Shepard NT, Telian SA. Practical Management of the Dizzy Patient. Lippincott Williams & Wilkins. 2002.
- MacDougall HG, et al. The video head impulse test: Diagnostic accuracy in peripheral vestibulopathy. Neurology. 2009;73(14):1134–1141.
- Kattah JC, et al. HINTS to diagnose stroke in the acute vestibular syndrome: Three-step bedside oculomotor examination more sensitive than early MRI DWI. Stroke. 2009;40(11):3504–3510.