This is the hidden cost of aminoglycoside antibiotics in India. These powerful drugs are lifesaving against serious infections-TB, sepsis, gram-negative bacterial infections.
But they destroy the vestibular system when used aggressively or prolonged. And in India, where these drugs are used liberally and often without vestibular monitoring, bilateral vestibulopathy is probably more common than doctors realize.
Here’s what you need to know about bilateral vestibulopathy: it’s different from regular vertigo, it’s often iatrogenic (caused by medical treatment), and with proper rehabilitation, patients CAN improve functionally.
What Is Bilateral Vestibulopathy?
Bilateral vestibulopathy (BV) means loss of vestibular function in BOTH ears (bilateral = both sides, vestibulopathy = disease of the balance system).
Your balance system has two main components: the vestibular apparatus in each inner ear. Under normal circumstances, these two sides work in balance. When you turn your head left, the left vestibular system increases signaling and the right side decreases-your brain integrates this asymmetric input to know which direction you’re moving.
When BOTH sides are damaged, the balance system can’t function in its normal way. Instead, you lose the ability to automatically stabilize your eyes during head movement. You can’t quickly sense whether you’re moving up, down, or sideways. Your brain has to rely on vision and proprioception (body position sense) much more heavily.
Key Point: Bilateral Vestibulopathy Feels Different From Unilateral Vertigo
This is crucial because many patients (and even some doctors) think all vertigo is the same. It’s not.
Unilateral vestibular loss (one ear damaged): Spinning vertigo, nausea, the world feels like it’s moving. Severely incapacitating acutely. But the brain compensates relatively well over 4-6 weeks because the healthy side can take over.
Bilateral vestibular loss (both ears damaged): NOT spinning vertigo (because both sides are equally affected, the brain doesn’t perceive asymmetric rotation). Instead, oscillopsia (world bouncing when walking), gait instability, falls, severe balance problems especially in dark or on uneven ground.
Patients often tell me: “I don’t feel dizzy, but I can’t walk. Everything bounces when I move.”
Symptoms of Bilateral Vestibulopathy, How to Recognize It
Oscillopsia, The Bouncing World
This is pathognomonic (characteristic) of bilateral vestibulopathy. When you walk or move, objects appear to bounce or jiggle. Your vision isn’t clear during head movement.
Why? Your eyes need vestibular reflexes to stay focused on a moving target while your head moves. The vestibulo-ocular reflex (VOR) normally stabilizes your eyes. When both vestibular systems are down, this reflex is lost. So reading becomes impossible while walking, watching your feet is difficult, videos are nauseating.
Patients describe it:
- “When I walk, the world jumps around”
- “I can’t see clearly when moving”
- “The ground seems to bounce under my feet”
- “I feel like I’m on a boat”
Gait Imbalance, Severe Balance Problems
The gait is characteristic. Patients walk carefully, narrowly, with a stiff body. They need to stabilize themselves. Their walking is worse:
- In the dark (can’t use visual compensation)
- On uneven ground (proprioceptive input unreliable)
- When turning head while walking
- When climbing stairs
Many patients report near-falls or falls. Disability can be severe.
Gaze Instability
When you look from side to side rapidly, your eyes don’t move smoothly. Patients describe difficulty reading, difficulty watching people’s faces. This is because the smooth eye movement and gaze-stabilization depend on vestibular function.
Vertigo Usually NOT Present
This is the critical differentiator. Unlike acute vestibular neuritis (one ear suddenly affected), bilateral patients usually DON’T report spinning vertigo. The deficit is symmetric-the brain doesn’t perceive rotation. Instead, they report imbalance and oscillopsia.
No Hearing Symptoms (Usually)
The vestibular system and hearing system are separate, though they coexist in the inner ear. Aminoglycosides (the main cause of BV) damage vestibular function more than hearing, so patients may have normal hearing despite severe vestibular loss. However, some hearing loss might occur.
Causes of Bilateral Vestibulopathy in India
Aminoglycoside Ototoxicity (THE Major Cause in India)
Aminoglycosides are antibiotics that are highly effective against serious gram-negative bacterial infections and TB. But they’re also notoriously vestibulotoxic.
Common aminoglycosides in India:
- Streptomycin: Used for TB (though less now with newer TB drugs). Potent vestibulotoxin.
- an ototoxic antibiotic: Used for serious gram-negative infections (sepsis, hospital-acquired infections). Common in ICUs.
- Tobramycin: Similar to an ototoxic antibiotic.
- Amikacin: For drug-resistant TB and serious infections.
- Netilmicin: Less vestibulotoxic than others but still risk.
Risk factors for aminoglycoside-induced bilateral vestibulopathy:
- Prolonged use: More than 2 weeks of therapy
- High cumulative dose: Total lifetime dose > 15 grams
- Renal failure: Impaired clearance means higher drug levels
- Concurrent use of other ototoxic drugs: NSAIDs, loop diuretics, vancomycin
- Age >60: Age increases vulnerability
- Dehydration: Increases drug concentration in ear
- Genetic susceptibility: Some people are genetically predisposed to vestibular damage
The Indian Problem: In India, TB treatment protocols typically include streptomycin, and ICU patients with sepsis often receive an ototoxic antibiotic. We should be monitoring vestibular function during treatment, but many centers don’t. Patients develop bilateral vestibulopathy and nobody realizes the connection until symptoms are severe.
Autoimmune Inner Ear Disease
Rare condition where the immune system attacks vestibular function. Can be bilateral. Associated with systemic autoimmune diseases. Requires specialized testing and typically corticosteroid treatment.
Bilateral Meniere’s Disease
Even rarer. Classic Meniere’s is unilateral, but bilateral Meniere’s exists. Much rarer than unilateral. Characterized by hearing loss, tinnitus, and episodic vertigo on BOTH sides.
Idiopathic Bilateral Vestibulopathy
Some patients develop bilateral vestibulopathy without clear cause. This is considered a diagnosis of exclusion after ruling out infections, autoimmune disease, and ototoxic drugs. The cause remains unknown.
CNS Disorders
Rarely, bilateral vestibular loss results from brainstem or cerebellar disease, though this is usually from central causes rather than peripheral vestibular pathology.
How Bilateral Vestibulopathy Is Diagnosed
Clinical Examination, The Video Head Impulse Test
This is THE key test for bilateral vestibulopathy. I do this in clinic:
While you watch my nose, I move your head side to side rapidly. Your eyes should automatically follow and stay fixed on my nose (vestibulo-ocular reflex). In bilateral vestibulopathy, your eyes can’t keep up-they slip off my nose. Your eyes are abnormal on BOTH sides.
This asymmetric finding is diagnostic of bilateral vestibulopathy.
Caloric Testing
The definitive test. Warm and cold water (or air) is introduced to the ear canal, stimulating the horizontal semicircular canals. A normal response is eye movements (nystagmus). Bilateral hypo-reflexia or areflexia (no response) confirms bilateral vestibular loss.
Finding: responses are reduced or absent on both sides.
Rotatory Chair Testing
More sophisticated testing where you sit in a rotating chair and your eye movements are tracked. The vestibulo-ocular reflex gain (normal ~1.0) is reduced bilaterally.
Videonystagmography (VNG)
Infrared video tracks eye movements in response to various stimuli. Helps document vestibular dysfunction objectively.
MRI of Brain (When Indicated)
If cause is unclear, MRI rules out central nervous system pathology. Required if autoimmune inner ear disease suspected.
Audiometry
Documents hearing status. Aminoglycoside damage may or may not affect hearing (vestibular more vulnerable). Normal hearing doesn’t rule out bilateral vestibulopathy.
Why Bilateral Vestibulopathy Is Missed
Several reasons this condition is underdiagnosed in India:
- No spinning vertigo: Patients don’t report classic “dizzy” symptoms, so vestibular disease isn’t suspected
- Attributed to age: Elderly patients with falls and imbalance are just written off as “old age”
- Attributed to neurological disease: Balance problems are sometimes thought to be stroke, Parkinson’s, or normal aging
- No documentation during aminoglycoside use: Vestibular monitoring not done, so cause-effect isn’t established
- Vestibular testing unavailable: Caloric testing requires special equipment not available in all clinics
- No clear treatment: Doctors hesitate to diagnose something they can’t cure, so diagnosis is avoided
Treatment of Bilateral Vestibulopathy, It’s Not About Medications
The Critical Point: There’s No Drug to Restore Vestibular Function
Unlike unilateral vestibulopathy where the healthy side can compensate and improve, bilateral vestibulopathy cannot be “fixed” by pills. The vestibular cells are damaged (usually permanently), and no medication restores them.
So treatment focuses on:
- Rehabilitation to maximize compensation
- Prevention of further damage
- Safety and fall prevention
- Optimizing vision and proprioception to compensate
Vestibular Rehabilitation Therapy (VRT), The Gold Standard
This is the cornerstone of treatment. VRT involves physical therapy exercises specifically designed to retrain the central vestibular system and improve gaze stability and balance.
Goals of VRT:
- Improve vestibulo-ocular reflex through gaze-stabilization exercises
- Improve balance and gait confidence through progressive balance training
- Reduce dependency on visual input
- Reduce falls and improve quality of life
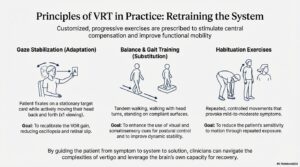
Key exercises:
- Gaze stabilization: Focusing on a fixed target while moving head side to side
- Dynamic balance exercises: Standing on one leg, tandem stance, walking with head turns
- Proprioceptive training: Balance on unstable surfaces, eyes closed, to improve sense of body position
- Habituation exercises: Repeated exposure to movements that trigger oscillopsia to reduce sensitivity
VRT typically requires 4-6 weeks of therapy (2-3 sessions per week) to show meaningful benefit. But functional improvement continues over months to years.
In India: VRT services are available at:
- Larger medical college hospitals with physiotherapy departments
- Private rehabilitation centers in metros
- Some ENT specialists trained in vestibular rehabilitation
Learn more about vestibular rehabilitation from the Vestibular Disorders Association..
Environmental Modifications
While undergoing rehabilitation:
- Remove tripping hazards from home
- Install handrails on stairs
- Improve home lighting
- Use mobility aids (walker, cane) if needed
- Avoid uneven surfaces until balance improves
- Don’t drive if oscillopsia is severe
Vision Optimization
Since vision becomes a critical compensatory mechanism:
- Ensure corrective lenses are up-to-date
- Good lighting is essential
- Avoid bifocals (complicate vestibular compensation)
No Role for Vestibular Suppressants
Medications like a vestibular suppressant or a vasodilator medication don’t help bilateral vestibulopathy because the problem isn’t overactive vestibular signaling (which suppressants address). The problem is absent signaling. Suppressants actually slow central compensation, so they’re generally avoided.
Vitamin D Supplementation
If deficient (common in India), vitamin D supplementation might support vestibular recovery. But evidence is limited.
The Prevention Story, Why This Matters in India
This is where I want to make the biggest impact. Bilateral vestibulopathy from aminoglycosides is largely preventable.
Key Prevention Strategies
1. Avoid aminoglycosides when safe alternatives exist
Modern TB drugs (isoniazid, rifampicin, pyrazinamide, ethambutol) are effective without the ototoxicity. Streptomycin use in TB is declining globally. In India, streptomycin should be used only in drug-resistant TB where alternatives are exhausted. Routine TB doesn’t need streptomycin.
2. For serious bacterial infections, use aminoglycosides judiciously
For gram-negative sepsis, an ototoxic antibiotic is often necessary. But:
- Use shortest effective duration possible
- Use extended-interval dosing () rather than three-times daily. Extended-interval dosing is less ototoxic
- Monitor renal function-avoid use in severe renal failure if possible
- Monitor vestibular function during prolonged use (caloric testing at baseline and during treatment)
- If vestibular symptoms develop, STOP immediately
3. Baseline and During-Use Vestibular Monitoring
Any patient receiving >2 weeks of aminoglycosides should have:
- Baseline caloric testing or head impulse test before starting
- Repeat testing every 1-2 weeks during treatment if prolonged
- Patient counseling on vestibular symptoms to watch for
Early detection of vestibular damage allows stopping the drug before complete bilateral destruction.
4. Educate TB patients taking streptomycin
If a TB patient MUST take streptomycin, they should:
- Be warned about vestibular side effects
- Report immediately if imbalance, oscillopsia, or difficulty walking develops
- Have baseline vestibular testing
- Not ignore balance symptoms as “just getting older”
5. Limit cumulative dose
Lifetime cumulative an ototoxic antibiotic dose should be <15 grams if possible. With TB and streptomycin, total dose should be limited. This requires dosage calculation and tracking.
Prognosis and Recovery in Bilateral Vestibulopathy
This is the realistic conversation I have with patients:
The bad news: The vestibular cells destroyed by aminoglycosides don’t regenerate. The damage is permanent. You won’t fully recover normal vestibular function.
The good news: With vestibular rehabilitation, most patients improve functionally. Many learn to walk independently, reduce fall risk, and resume activities. The brain is remarkably adaptable.
Timeline:
- First 2-4 weeks: acute compensation, some spontaneous improvement as brain adjusts
- Weeks 4-12: vestibular rehab starts showing benefits
- 3-6 months: significant functional improvement in most patients
- 6-12 months: continued gradual improvement, though some plateau at 6 months
- Beyond 1 year: plateau reached in most, but quality of life is often substantially better than immediately post-diagnosis
Factors predicting better outcomes:
- Younger age at diagnosis
- Earlier treatment/rehabilitation initiation
- High motivation for therapy
- Good overall health and fitness
- No concurrent neurological disease
Bilateral Vestibulopathy vs. Unilateral, Key Differences
| Feature | Unilateral Vestibulopathy | Bilateral Vestibulopathy |
|---|---|---|
| Presentation | Acute spinning vertigo, severe initially | Gradual imbalance, oscillopsia, no spinning sensation |
| Acute Severity | Extremely incapacitating acutely | Less acute distress, more chronic disability |
| Natural Compensation | Good. Brain learns from healthy side. Often 80% recovery without therapy | Poor. No intact side to compensate. Severe disability without rehabilitation |
| Oscillopsia | Rare | Hallmark symptom |
| Gait Impact | Usually improves significantly on own | Requires intensive rehabilitation |
| Long-term Disability | Most achieve good functional recovery | Many have persistent balance limitations |
| Video Head Impulse Test | Abnormal on ONE side | Abnormal on BOTH sides |
Frequently Asked Questions About Bilateral Vestibulopathy
Q1: I took TB drugs years ago. Can I develop bilateral vestibulopathy now?
Unlikely. Vestibular damage from aminoglycosides occurs during the treatment period or shortly after. Delayed onset years later is rare. However, if you’re now noticing balance problems, see an ENT specialist for proper evaluation.
Q2: If I have bilateral vestibulopathy, will I go deaf?
Not necessarily. Vestibular damage and hearing damage are separate. Streptomycin typically damages vestibular function more than hearing. Some aminoglycosides affect both, but hearing loss isn’t inevitable. Have your hearing tested to know your status.
Q3: Can I drive with bilateral vestibulopathy?
During acute stages or with severe oscillopsia, no-it’s unsafe. As you improve with rehabilitation, driving might become possible if oscillopsia resolves. But oscillopsia while driving is dangerous. Work with your therapist to determine when safe.
Q4: My parent has bilateral vestibulopathy from old TB treatment. Is there anything that can help?
Yes. Vestibular rehabilitation can improve function even years after damage occurred. It’s never too late to start. Additionally, physical therapy for balance and strength helps. Fall prevention measures are critical. Talk to an ENT specialist about rehabilitation options.
Q5: Is there any medication that restores vestibular function?
No. No medication restores damaged vestibular cells. This is why rehabilitation (training the brain to compensate) is the only real treatment.
Q6: Can stem cells or regenerative medicine help bilateral vestibulopathy?
Research is ongoing, but regenerative approaches aren’t standard treatment in India yet. For now, vestibular rehabilitation is your best option.
Q7: Will bilateral vestibulopathy get worse over time?
The vestibular damage doesn’t typically progress (it happened from the initial insult-the aminoglycoside). However, aging-related balance decline happens on top of this. With proper rehabilitation and exercise, many patients maintain or improve function for years.
Q8: My doctor says my balance problems are from aging, not bilater vestibulopathy. How do I know which?
Age-related balance decline is gradual and affects many functions (strength, vision, proprioception). Bilateral vestibulopathy specifically causes oscillopsia and abnormal head impulse tests. Proper vestibular testing (caloric, head impulse) can differentiate. Get tested by an ENT specialist to be sure.
The Aminoglycoside Crisis in India, A Call for Better Monitoring
I’ll be direct: we have an unrecognized epidemic of iatrogenic (medically caused) bilateral vestibulopathy in India. Every year, thousands of TB patients are treated with streptomycin. Thousands of ICU patients receive an ototoxic antibiotic. Many develop vestibular damage that’s never recognized or properly managed.
The solution requires changes at multiple levels:
- For clinicians: Monitor vestibular function during prolonged aminoglycoside use. Teach patients to report balance symptoms.
- For hospitals: Establish vestibular monitoring protocols for patients on aminoglycosides >2 weeks.
- For TB programs: Reduce streptomycin use where modern alternatives exist.
- For patients: If taking these drugs, report any balance symptoms immediately. Don’t wait.
- For rehabilitation centers: Expand vestibular rehabilitation services, especially in tertiary centers.
Key Takeaways About Bilateral Vestibulopathy
- Bilateral vestibulopathy causes oscillopsia and severe balance problems, NOT spinning vertigo
- Aminoglycosides (especially streptomycin, an ototoxic antibiotic) are the leading preventable cause in India
- Diagnosis requires vestibular testing (head impulse test, caloric testing)
- Treatment is vestibular rehabilitation-no medication restores function
- Functional improvement is possible with proper therapy even though complete recovery doesn’t happen
- Prevention through careful aminoglycoside use and monitoring is critical
- If you’re at risk (TB patient, ICU patient on aminoglycosides), advocate for vestibular monitoring
Balance Problems After Antibiotic Use? Get Evaluated
Dr. Prateek Porwal, DNB (ENT), MBBS provides comprehensive vestibular evaluation and rehabilitation guidance for bilateral vestibulopathy at Prime ENT Center, Hardoi.
Call: 7393062200
Proper diagnosis and rehabilitation planning for vestibular disorders.
Also read: BPPV શું છે? કાનમાં પથરી ખસવાથી ચક્કર આવવું
📋 Table of Contents
- What Is Bilateral Vestibulopathy?
- Key Point: Bilateral Vestibulopathy Feels Different From Unilateral Vertigo
- Symptoms of Bilateral Vestibulopathy, How to Recognize It
- Oscillopsia, The Bouncing World
- Gait Imbalance, Severe Balance Problems
- Gaze Instability
- Vertigo Usually NOT Present
- No Hearing Symptoms (Usually)
- Causes of Bilateral Vestibulopathy in India
- Aminoglycoside Ototoxicity (THE Major Cause in India)
- Autoimmune Inner Ear Disease
- Bilateral Meniere’s Disease
- Idiopathic Bilateral Vestibulopathy
- CNS Disorders
- How Bilateral Vestibulopathy Is Diagnosed
- Clinical Examination, The Video Head Impulse Test
- Caloric Testing
- Rotatory Chair Testing
- Videonystagmography (VNG)
- MRI of Brain (When Indicated)
- Audiometry
- Why Bilateral Vestibulopathy Is Missed
- Treatment of Bilateral Vestibulopathy, It’s Not About Medications
- The Critical Point: There’s No Drug to Restore Vestibular Function
- Vestibular Rehabilitation Therapy (VRT), The Gold Standard
- Environmental Modifications
- Vision Optimization
- No Role for Vestibular Suppressants
- Vitamin D Supplementation
- The Prevention Story, Why This Matters in India
- Key Prevention Strategies
- Prognosis and Recovery in Bilateral Vestibulopathy
- Bilateral Vestibulopathy vs. Unilateral, Key Differences
- Frequently Asked Questions About Bilateral Vestibulopathy
- Q1: I took TB drugs years ago. Can I develop bilateral vestibulopathy now?
- Q2: If I have bilateral vestibulopathy, will I go deaf?
- Q3: Can I drive with bilateral vestibulopathy?
- Q4: My parent has bilateral vestibulopathy from old TB treatment. Is there anything that can help?
- Q5: Is there any medication that restores vestibular function?
- Q6: Can stem cells or regenerative medicine help bilateral vestibulopathy?
- Q7: Will bilateral vestibulopathy get worse over time?
- Q8: My doctor says my balance problems are from aging, not bilater vestibulopathy. How do I know which?
- The Aminoglycoside Crisis in India, A Call for Better Monitoring
- Key Takeaways About Bilateral Vestibulopathy
- Balance Problems After Antibiotic Use? Get Evaluated
- Related Articles
- References
Related Articles
Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice, diagnosis or prescribing guidance. Consult Dr. Prateek Porwal at Prime ENT Center, Hardoi for personalised treatment.
References
- Strupp M, et al. Bilateral vestibulopathy: Diagnostic criteria consensus document of the Classification Committee of the Bárány Society. Journal of Vestibular Research. 2017;27(4):177–189.