If I had to choose one thing that matters most for vestibular neuritis recovery, it’s not the medication. It’s not the steroids. It’s vestibular rehabilitation exercises. I’m going to explain exactly why, and then I’m going to give you specific exercises you can do at home starting this week.
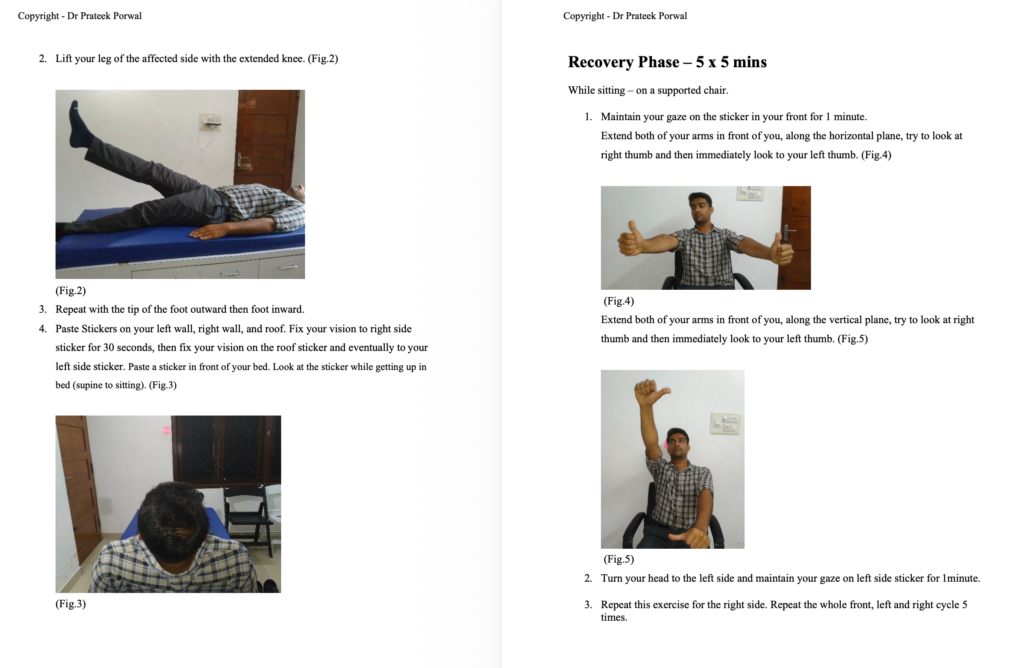
Vestibular Rehabilitation After Neuritis Is Critical
Let me explain the neuroscience first. When your vestibular nerve is damaged, your brain receives abnormal or incomplete balance information. Your brain’s job is not to restore the damaged nerve-that happens on its own as inflammation subsides. Your brain’s real job is to learn to work around the damaged input. This is called central vestibular compensation.
This compensation doesn’t happen passively. It requires repetition. It requires movement that provokes the damaged balance system. It requires exercises that challenge balance and force the brain to reorganize.
A patient who rests completely will have slower compensation. A patient who does vestibular rehabilitation exercises will compensate faster and more completely. This is not theory-this is evidence-based. Multiple studies show vestibular rehabilitation improves outcomes dramatically compared to no rehabilitation.
I often tell patients: the vestibular suppressant medication I prescribe helps you survive the acute phase. But the exercises are what makes you recover.
The Problem With Vestibular Suppressants: Why I Limit Them
Cinnarizine, betahistine (Vertin), antiemetics-these medications help control symptoms acutely. But they suppress the vestibular system’s ability to send signals to the brain. If you use these too long, you delay compensation.
This is why I tell patients: use these medications for the first few days if needed to control the severe vertigo. But by week 2, I want you off them. You need your damaged balance system to send whatever signals it can so your brain can learn from them and compensate.
A patient who stays on vestibular suppressants for months will have prolonged symptoms. A patient who stops them by week 2-3 and starts exercises will recover faster.
The Three Essential Types of Vestibular Rehabilitation Exercises
I recommend three categories of exercises for vestibular neuritis recovery:
Most of my patients, which you will also see in your clinic will have these features-
- 1. Vertigo/Dizziness
- 2. Anxiety/Depression
- 3. Vomiting/vegetative symptoms
- 4. Imbalance
- 5. Disturbed quality of Life
- 6. Recurrences
- Give most of your time to symptoms from 2 to 6.
Also next step should be to counsel them –
- • Be familiar with them, ask about their job, family and day to day activities,
- • Tell them about yourself, make them comfortable.
- • Tell them that you understand the disease, patients feeling and that you care for them.
- • Identify their aggravating factors, concomitant diseases like HTN, DM2 etc.
- • Habits – Alcohol, smoking etc
- • Dietary habit modifications – drink 2 liters of water, low calorie intake, decent breakfast, light lunch, stop coffee, chocolate etc
- • Tips to control stress – Tai chi and yoga.
1. Gaze Stabilization Exercises (VOR-Vestibulo-Ocular Reflex)
This is the most important exercise. It trains your vestibular system and eyes to work together to keep your gaze stable when your head moves.
Here’s how to do it:
- Sit comfortably and pick a target to focus on-a letter on a chart, a mark on the wall, anything specific
- Keep your eyes locked on the target while slowly moving your head side to side
- Keep it slow at first-maybe one head movement per second
- Do 20 repetitions, 3 times daily
- Once this is comfortable (after a few days), add vertical head movements (up and down)
- Then add diagonal movements
- Gradually increase the speed of head movement
The goal: your eyes should stay locked on the target while your head moves. Your eyes should not jerk or lose focus. This exercise strengthens the remaining vestibular system’s ability to control eye movement.
You should feel mild dizziness with these exercises-that’s normal and good. If the dizziness is severe and nauseating, slow down or reduce intensity.
2. Head Movement Exercises
These get progressively harder:
Week 1-2 (Seated):
- Slow head movements side to side, up and down, and in circles
- 10 repetitions each direction, 2 times daily
- Mild dizziness is expected
Week 2-3 (Standing):
- Do the same head movements while standing, holding onto something stable
- This adds balance challenge
- If unstable, keep hand on surface
Week 3-4 (Dynamic Walking):
- Walk forward slowly while moving your head side to side
- 5 minutes, once daily
- This really challenges the vestibular system
3. Balance Training and Habituation
As vertigo improves (after week 3-4), add balance challenges:
- Stand on one leg, 30-60 seconds, 3 times daily
- Stand with feet together and eyes closed (carefully, with someone nearby), 30 seconds
- Tandem stance (heel-to-toe), 30 seconds
- Walk heel-to-toe in a straight line
- Use a balance board if available
These exercises train your other balance systems (vision, proprioception) to take over as the vestibular system recovers.
Vestibular Rehabilitation After Neuritis
The Cawthorne-Cooksey Exercises: I don’t use and don’t advice these exercises.
My Protocol Dr Prateek Porwal VRT for Vestibular Neuritis
Mine is three sets of exercise’s, namley Acute Phase where patient is not able to stand or sit and is lying in bed, Recovery Phase where patient is able to sit and do sitting exercises and last is strentging set where the patient is able to walk and do gaze exercises. I will attach a youtube video on this topic where i have taught 200 ENT doctors about my VRT protocol.
How to Progress Exercises Safely
Key principle: exercises should cause mild to moderate dizziness, not severe spinning vertigo.
If exercises cause only mild symptoms, they’re likely too easy-progress to the next level. If they cause severe nausea and spinning, they’re too hard-reduce difficulty.
Progression looks like this:
Week 1-2: Gaze stabilization seated, gentle head movements seated. 10-15 minutes total, 2-3 times daily.
Week 2-3: Gaze stabilization standing, head movements standing, add walking gaze exercise. 15-20 minutes total, 2 times daily.
Special Complaints
How to get up from a chair:
1. Place your hands on the chair’s arms.
2. Bend forward your trunk and lift yourself, pushing on the chair’s arms.
3. Now, get up looking at the front.
4. Wait for a few seconds before walking.
How to pick an object from the floor:
1. Push the object near a table or any support.
2. Using the table as support, bend your knees, and pick the object.
3. Lift yourself using the table for support.
How to get out of bed:
1. Turn yourself to one side.
2. Move your legs over the side of the bed.
3. Lift your trunk slowly.
4. Sit fixating in front of you, wait for few seconds before standing up.
Home-Based Versus Formal Physiotherapy
Many patients ask: do I need a physiotherapist, or can I do these exercises at home?
In my experience in Hardoi, many patients don’t have easy access to formal vestibular physiotherapy. Home-based exercises following a structured protocol work well. I provide detailed written instructions or videos and patients follow them at home.
However, formal physiotherapy has advantages:
A good physiotherapist can assess your specific deficits and customize exercises. They can watch your form and correct technique. They can progress you appropriately and quickly. They can motivate you on days you’re discouraged.
If formal physiotherapy is accessible to you, I recommend it, particularly if home exercises aren’t progressing well.
If not accessible, home exercises work-with commitment and consistency.
Why Patients Stop Exercising (And Why They Shouldn’t)
I see this pattern frequently: patient feels better around week 3-4. Symptoms have improved dramatically. Patient thinks “Great, I’m recovered” and stops doing exercises. Then recovery plateaus or setbacks occur.
This is a mistake. The brain is still reorganizing during weeks 4-12. The exercises drive this reorganization. Stopping too early means incomplete compensation.
I tell patients: keep doing exercises even as you feel better, especially as you feel better. The brain is working hard during this phase. The exercises are most important now, not when you were severely symptomatic.
Most patients who do exercises consistently through week 12 recover completely. Patients who stop early often have residual symptoms.
Specific Timeframes and Expected Results
Week 1: Starting exercises helps survivability of acute phase. Expect no major improvement yet.
Week 2: Vertigo improving. Exercise tolerance increasing. Some patients report 50% improvement.
Week 3: Major improvement often. Dizziness much less. Can do more complex exercises.
Week 4: Functional recovery often substantial. Back to light activities for most.
Week 6: Most patients feeling near-normal for many activities. Residual symptoms with specific movements only.
Week 8-12: Complete or near-complete functional recovery for most.
Beyond Week 12: Fine-tuning continues. Some patients improve further out to 6 months.
That’s the typical timeline with dedicated exercises. Without exercises, recovery is slower and less complete.
Results: The Evidence for Vestibular Rehabilitation
Studies consistently show patients who do vestibular rehabilitation recover faster and more completely than those who don’t. The difference is significant.
One key study showed patients doing home vestibular rehabilitation exercises had complete symptom resolution in an average of 6 weeks. Untreated patients took much longer to achieve the same recovery.
At my clinic, I see this repeatedly. Patients who commit to exercises do dramatically better. Patients who don’t do exercises have prolonged symptoms.
Special Situations
Patients with anxiety: Some patients develop anxiety about dizziness, which prevents them from doing exercises. They fear the dizziness will become severe again. I discuss this openly and sometimes refer for psychological support. Gradual, supported exercise helps overcome the anxiety.
Elderly patients: Older patients sometimes worry about falls. Using equipment for support (chair, walker) makes exercises safer. Still important to do them.
Patients with vision problems: Gaze stabilization exercises require visual targets. Blind patients or those with poor vision need modifications. I work with them to adapt exercises.
Patients with other balance conditions: Some patients have other causes of imbalance (diabetes neuropathy, etc.). Vestibular rehab still helps but may be progressed more slowly.
How I Monitor Progress
I see patients back at 2 weeks and 4 weeks to assess progress. I look for:
Symptom improvement-how much better do they feel?
I always check for the initial disorder progression, like if its vestibular neuritis then i always look for spontaneous nystagmus and also check that it follows the Alexanders law or now ? And whther the nystagmus intensity has reduced or not.
Exercise tolerance-can they do harder exercises without severe symptoms?
Functional recovery-can they do work, drive, play with their children?
Head impulse test improvement-is the vestibular reflex recovering?
If progress is good, I encourage continuation of current exercises and progression. If progress is slow, I look for barriers and adjust the program.
Frequently Asked Questions
Q: How long until I can stop doing exercises?
A: Continue formal exercises through week 12, then transition to maintenance exercises (2-3 times per week). Many patients continue modified exercises indefinitely-they’re simple and help prevent symptom recurrence.
Q: What if exercises make me feel worse?
A: You’re doing too much intensity. Reduce difficulty or speed. Mild dizziness is good. Severe spinning is too much.
Q: Can I exercise if I’m still on vestibular suppressants?
A: Ideally not. Suppressants block the signals needed for exercise benefit. I recommend stopping suppressants by week 2 before starting serious rehabilitation.
Q: Do I need equipment?
A: Not for basic exercises. A stable chair, wall, and clear space are enough. Balance boards are helpful but not essential.
Q: Can I exercise outside, or only indoors?
A: Outside works too, though initially indoors is safer in case of falls. Once stable, outdoor walking with head movements is great rehabilitation.
What to Do Starting Now
If you have vestibular neuritis, start vestibular rehabilitation immediately. Don’t wait. The sooner you start, the faster you recover. Even simple gaze stabilization exercises in the acute phase help prime the brain for compensation.
Follow the progression I outlined. Be consistent. Expect mild dizziness during exercises-that’s the point.
Most importantly: don’t stop exercises when you feel better. That’s when they matter most.
If you need guidance, call Prime ENT Center at 7393062200 or WhatsApp https://wa.me/917393062200. I can assess your progress, provide detailed exercise instructions, or refer for formal physiotherapy if needed. My goal is your complete recovery-and with dedicated rehabilitation, that’s what most patients achieve.
Related Articles
- Vestibular Neuritis: Complete Guide to Understanding and Recovery
- Vestibular Neuritis Recovery, Timeline and Exercises
- Steroids for Vestibular Neuritis, Do They Really Work?
- Vestibular Neuritis vs Labyrinthitis, Key Differences
Medical Disclaimer: This article is for educational purposes only. It does not constitute medical advice or prescribing guidance. All medications mentioned should only be taken under the direct supervision of a qualified physician. Specific doses, durations, and drug choices depend on your individual clinical condition and must be determined by your treating doctor. If you experience severe symptoms, please seek immediate medical attention.
About the Author
Dr. Prateek Porwal is an ENT Surgeon at Prime ENT Center in Hardoi, UP with 13 years of experience, holding MBBS (GSVM Medical College), DNB ENT (Tata Main Hospital), and CAMVD (Yenepoya University). He is the originator of the Bangalore Maneuver for Anterior Canal BPPV and has published research in Frontiers in Neurology and IJOHNS. functional recovery.
Contact:
Prime ENT Center, Hardoi, UP
Phone: 7393062200
WhatsApp: https://wa.me/917393062200
Website: drprateekporwal.com